Layla Siraj, AB
Harvard Medical School; Program in Health Sciences & Technology, Harvard Medical School & Massachusetts Institute of Technology, Boston, MA 02115
Correspondence should be addressed to L.S. (layla.siraj@gmail.com)

Clay illustration by Lily Offit; Photographed by Ben Denzer
INTRODUCTION
I have my own version of Bobby’s death tie: 3 inch wedges[1]. I thought to myself that morning as I turned around to slip the beeper into my bag, that there was no way we could get paged this early, on the second day after group borborygmi. Yet, the death wedges prevailed, and, though not pleased at the thought of missing pathology (why couldn’t it be biochem!), I ran[2] to the Brigham to meet my first patient.
[1] Surprisingly, not death for my ankle: I have yet to put myself in a walking boot wearing heels. Sneakers, on the other hand...
[2] Yes, in those wedges. A benefit of training as a figure skater!
CLINICAL BACKGROUND
The decedent was a 72-year-old obese female. Her past medical history was significant for Parkinson’s disease, an umbilical hernia, and a hiatal hernia. The hiatal hernia had been treated with a laparoscopic type III mesh placement as well as a Nissen fundoplication on September 6, 2016.
The patient presented to Faulkner hospital on September 18, 2016, with sharp and crampy abdominal pain. She was found to have a ventral hernia, which was confirmed by CT. CT also revealed findings concerning for strangulation. The patient underwent emergent laparotomy to reduce and repair the hernia. The surgery and recovery were uneventful until post-op day 1, September 19, 2016, when the patient went into respiratory arrest. The code team arrived and had difficulty intubating, as the patient had two prominent upper canines that blocked the passage of the tube. After the tube was placed, the patient’s oxygen saturation remained between 85-88%. The decision was made to re-intubate. During the process of re-intubation, the patient entered pulseless electrical activity and fluid could be seen in the back of the oropharynx. The reintubation was completed and the patient’s oxygen saturation climbed to 94%; however, she had persistent arrhythmia and could not be resuscitated. She expired at 5:19 PM on September 19, 2016. Consent for an unrestricted autopsy at Brigham and Women’s Hospital was given by the decedent’s daughter. The goals of the autopsy were to elucidate the reason for the respiratory arrest. Possibilities included, but were not limited to, a pulmonary embolism from a deep vein thrombus, or a myocardial infarction.
GROSS PATHOLOGY
At autopsy, the patient was identified by a hospital ID bracelet on the left wrist and an ID tag attached to the right great toe. External examination of the patient revealed a female with grey hair, brown eyes with arcus senilis, and 0.5 cm pupils bilaterally. There was a plethora of evidence of medical intervention, including the following: two sets of electrical pads, one attached to her left anterior chest wall and upper back, and the other attached to her left superior abdomen; an endotracheal tube; access lines on the dorsal left hand and left chin; a bandage in the antecubital fossa; EKG pads on the right shoulder, right and left superior chest, right superior abdomen, left central abdomen, bilateral thighs, and bilateral ankles; a midline, 8.5 cm stapled incision site that was well-approximated, clean, and dry; laparoscopy port sites on the superior midline abdominal wall (0.7 cm), upper right abdominal wall (1.9 and 1.3 cm), left abdominal side wall (0.9 cm), and left anterior abdominal wall (1.2 and 0.8 cm). Further external examination revealed two abrasions near the xyphoid process (4.6 and 3.2 cm), ecchymoses bilaterally on the anterior thighs. Also noted was a 10.5 x 0.6 cm white fibrotic region of the skin on the right superior buttock.
After the organ block was removed, the thoracic cavity was examined and determined to be unremarkable. The thoracic cavity contained small lungs with increased weight (right lung 620 g, nl 360-570 g; left lung 540 g, nl 325-480 g). No pulmonary emboli were seen in the main pulmonary artery or the arteries of the left and right lungs. There was no grossly evident obstructing material or mucous in the lumina. The mucosa itself was uniform and hyperemic. The right lung was adhered to the diaphragm and esophagus at the esophageal hiatus, and there was significant fibrosis surrounding the adhesions. After sectioning, the lungs were dark red and non-crepitant, but no areas of consolidation were found. The bronchiolar tree was attenuated at the periphery. There was 150 mL of serosanguinous pleural fluid in the right pleural cavity and no fluid found in the left pleural cavity. The trachea was patent and showed no signs of upper airway obstruction. There were petechiae (up to 0.2 cm) present on the larynx between the true and false vocal folds and inferior to the true vocal folds. The thyroid gland (28.5 g, nl 30-70 g) was small but otherwise unremarkable.
Apart from its smallness (230 g, nl 250-300 g), the examination of the heart proved to be unremarkable. The ventricles were unremarkable, and no areas of recent or remote myocardial infarction were seen upon sectioning of the ventricles or triphenyltetrazolium chloride stain. The tricuspid, pulmonary, mitral, and aortic valves were unremarkable. The coronary vessels were patent, and there was no atherosclerosis of the aortic root. Dissection and sectioning of the coronary arteries revealed no thrombi. The aortic arch contained no atherosclerosis.
Next, we progressed to the abdomen. There was no ascites noted. The esophagus and stomach were adhered to the diaphragm at the esophageal hiatus. The stomach was fully expanded with air. Inside the stomach were 5 undigested pills, and another 2 undigested pills in the proximal duodenum. Each of the pills was 0.5 cm in diameter, orange-yellow, and had a ‘T’ inscribed on one surface. A google search[3] revealed a match with 325-mg enteric-coated aspirin tablets, which had previously been prescribed to the patient. According to the medical record, the patient was not taking these pills in the hospital. The pyloric sphincter was thickened (0.7 cm in greatest wall thickness. The examination of the small and large bowel demonstrated fecal contents, and there were no obstructions or ischemic segments of intestine identified. The appendix (8.1 cm in length x 0.6 cm in diameter) was present and unremarkable in appearance. The liver (1150 g, nl 1200-1400), was slightly small and showed evidence of autolytic changes. The gallbladder was not present. The pancreas and the spleen (75 g, nl 110-170) were both soft and cohesive consistent with early autolysis.
There was minimal atherosclerosis present in the abdominal aorta near the bifurcation into the common iliac arteries. The right and left renal arteries were patent. The kidneys (right 65 g, left 70, g, nl 115-155) were small, and both contained cortical retention cysts. The cut surfaces of the kidneys demonstrated intact corticomedullary junctions. The adrenal glands (right 9.4 g, left 13.5 g, nl 5-6 g) were large but otherwise unremarkable. The ureters were patent. The bladder had a white mucosal surfaces and a pink glistening peritoneal surfaces. The uterus and ovaries were unremarkable. The great saphenous veins were patent bilaterally, and there was no evidence of thrombosis.
The brain (1110 g, nl 1200-1300 g) and spinal cord were removed and sent to Neuropathology to examine due to her Parkinson’s disease. The findings were not pertinent to the cause and manner of death, which was the focus of this autopsy.
Taken together, the gross autopsy suggests that the cause of death in this patient, a 72-year-old woman status post ventral and hiatal hernia repair surgeries, was most likely an acute post-operative aspiration event, which was exacerbated by atelectasis, post-surgical adhesions between the esophagus, diaphragm, and right lung, and an enlarged and dilated stomach and a right pleural effusion, all of which led to respiratory distress that was complicated by a difficult intubation. In addition, there was evidence of gastroparesis and ileus, given the 7 undigested pills present in the patient’s stomach and proximal ileum. There was no indication of myocardial infarction, no gross or microscopic evidence of pulmonary emboli, upper airway obstruction, or coronary artery thrombi.
[3] Dr. Google comin’ in clutch.
MICROSCOPIC PATHOLOGY
A thorough examination of the ventricles of the heart revealed no signs of ischemia. No thrombi were seen in the coronary arteries. There was mild atherosclerosis with 10% mural compromise.
A histological examination of the lungs revealed vascular congestion and focal extravasation of red blood cells into alveoli, which is consistent with sudden death and resuscitation efforts. Rare bone marrow emboli were seen bilaterally in small vessels. There were rare, scattered foci of bacteria, squamous debris, and polarizable material in the alveoli, consistent with aspiration. There was no reaction around these foci of aspiration, suggesting that the aspiration event occurred either shortly pre-mortem or in the peri-mortem period. The large bronchi exhibit focal acute and chronic inflammation. There were no signs of aspiration in the trachea. The larynx exhibited subepithelial hemorrhage.
The muscular hypertrophy of the pylorus was confirmed histologically with trichrome staining. There was also evidence of submucosal chronic inflammation.
Microscopic investigation of the esophagus and paraesophageal soft tissue found extensive hemorrhage, fibrosis, and granulation tissue, all of which are consistent with a healing surgical site. There was no evidence of infection.
Examination of the kidneys microscopically showed congestion in small vessels. The spleen also had signs of congestion, but there were no other pathological abnormalities noticed. The liver was devoid of pathological abnormalities.
CLINOPATHOLOGICAL CORRELATIONS
Unlike in the third portion of our course, cancer is not the answer; instead, the answer is everything hernia.
Twelve days before presenting for her final hospital admittance, the decedent underwent emergent repair for a hiatal hernia. This was not our patient’s first hernia: she had previously presented with an umbilical hernia, which reveals general muscle weakness; additionally, the patient was well over the age of 50 and was obese, both of which are risk factors for hiatal hernias. A Nissen fundoplication with a laparoscopic type III mesh placement was performed to correct the defect and prevent a further hiatal hernia; however, this measure may have been a cause in her demise. Nissen fundoplications have been known to cause “gas-bloat syndrome,” which comprises a variable and not clearly defined set of complaints and which is assumed to result from an inability to vent gas from the stomach into the esophagus (Richter, 2013). This, along with difficulties in tube placement, may have contributed to the distended stomach filled with air noted in the gross pathological portion of the autopsy. Some gas-bloat syndrome patients also have issues with delayed gastric emptying, which would be consistent with the undigested pills in the patient’s stomach and proximal duodenum. The thickened pyloric sphincter also contributes to this difficulty in gastric emptying.
Fibrotic adhesions were found between the esophagus, the diaphragm, and the right lung. These are most likely a direct result of the Nissen fundoplication surgery, and this reduced the ability of the right lung to expand and of the diaphragm to maintain its full range of motion, decreasing the maximal volume of the lungs further.

Adhesions are no joke. Except in this e-card.
The adhesions and the gas-bloat syndrome symptoms may have led to increased difficulty of passages of boluses through the gastrointestinal tract. That, combined with the increased age, the size of the patient, and her past multiple pregnancies, leading to weakness of the abdominal wall, aided in the formation of her ventral hernia. This was the cause of her abdominal pains, which caused her to present to the hospital on September 6, 2016.
The patient then underwent an emergent surgery to repair the ventral hernia due to findings concerning for strangulation. Atelectasis, a partial collapse of a lung, is a common complication during surgery (“What Causes Atelectasis?”, 2012). In the gross examination of the lungs, the bronchi were found to be attenuated at the periphery, a finding that is consistent with atelectatic lungs. Furthermore, the pleural effusion noted in the right lung supports the clinical diagnosis of post-surgical atelectasis and would further reduce the expansion potential of the lung. This is consistent with the results of the gross pathological examination of the lungs, which revealed that the lungs were both smaller and heavier than normal limits. A pleural effusion was also noted in the autopsy; pleural effusions due to regional inflammation after surgery are a common complication in older patients (Lawrence et al, 1996).
Aspiration can occur in patients recovering from anesthesia. Anesthesia can weaken the autonomic regulation of the pharynx; because of this, aspiration events have happened, although they are not exceedingly common (Asai, 2004).
The polarizable material found in the microscopic pathology of the lung, combined with the squamous debris and scattered foci of bacteria, point to aspiration of the contents of the stomach, which, as we will recall, contained five undigested pills. Additionally, the lack of inflammation or reaction around the aspirated foci point to this event as the cause of death, as it must have occurred in the immediate pre-mortem period. The aspiration event is the likely cause of death, especially considering the exclusion of myocardial infarction from the triphenyltetrazolium chloride stain and physical examination as well as the lack of evidence of deep vein thrombi.
SUMMARY OF CAUSE OF DEATH
The reduced size of her lungs, from the atelectasis, pleural effusion, and adhesions, all of which resulted from her previous surgical repair for her hiatal hernia, were implicated in the immediate events leading to the patient’s expiration. Due to a thickened pyloric sphincter and delayed gastric emptying from the Nissen fundoplication, the patient was unable to digest pills taken preceding her hospital visit. The patient underwent an aspiration event the morning after her ventral hernia repair. This, combined with the already decreased lung volume, led to the respiratory arrest. The intubation most likely reached the stomach on first effort due to the excessive amount of air present. The patient then entered pulseless electrical activity due to her hypoxia, and she expired.

When lungs can’t expand fully, bad things happen.
THE MORE YOU KNOW
While complications from hernia repair led to our patient’s ultimate expiration, she avoided an issue that plagues mesh hernia repairs: infection. Mesh-related infections in hernia repairs have a reported incidence of between 1%-8% (Falagas and Kasiakou, 2005). Indeed, nosocomial infection is the fourth leading cause of death for American hospital patients with 2 million cases annually (Wenzel, 2007). Out of these, 60-70% are associated with an implantation of a medical device (Bryers, 2008). One of the main culprits of the infections associated with implantation of devices such as mesh during hernia repair or orthopaedic replacements is biofilm formation (Choi et al, 2012). My brief foray into materials science[4] and surgical research was focused on this field; we engineered a patch derived from organic collagen and seeded with human mesenchymal stem cells to, among other aims, thwart biofilm formation on two fronts. Firstly, the alginate portion of patch would degrade over time, decreasing the nutrient source and surface area for biofilm formation. Additionally, the human mesenchymal stem cells seeded upon the patch promote neovascularization, which allows for greater immune system recruitment and destruction of biofilms (Ayala et al, 2015). Biofilms are cool, bacteria are cool, and the way that bacteria have evolved to work together is incredible, kinda spooky, and has important implications on the evolutionary history of multicellularity as well as potential clinical applications.
Let’s back up a second - what exactly are biofilms? Biofilm, a term coined in 1978 though the discovery of these structures’ existence dates back to the 17th century (Banthia et al, 2011), refers generally to a multicellular community of microorganisms encased within an extracellular matrix, invariably involving multiple species (Lopez et al, 2010). This extracellular matrix protects the encased bacteria from antibiotics and other methods of destruction, and in these states biofilms and their biological components can persist in the body for long periods of time. These films are present almost everywhere, from our teeth in the form of dental plaques to ships and pipes and even in geothermal vents.
Though Antoine van Leeuwenhoek first noted the existence of biofilms in 1684, prior to 1978 the main research focus on bacteria was in planktonic (single and free-floating) form. This was due to the assumption that this was the natural state of most bacteria (Branda et al, 2005). However, in a groundbreaking Scientific American paper in 1978, Costerton et al asserted that most bacteria in natural environments adopt a sessile, multicellular form via a bacterial glycocalyx that allow the cells to stick to each other and anchor themselves in a film (Costerton et al, 1978).
Biofilm formation has now been studied in the lab through the development of techniques conducive to their growth, such as flow cells, liquid-air interfaces, and submerged films, and several general stages of biofilm formation have been identified (Branda et al, 2005)[5]. Initiation happens when microorganisms interact with a surface and each other. Once a critical mass has been reached, the biofilm maturation process begins with the production of an encasing extracellular matrix. Different species or mixes of species produce different extracellular components - Other maturation events include the formation of “persister” cells, which are dormant cells that are essentially invulnerable (metabolically inactive, exhibiting multidrug resistance) and are important to the survival of biofilms (Lewis, 2008). Despite the generality of these steps, biofilms can be incredibly diverse. Even small changes in the surrounding environment can lead to significant differences in the extracellular makeup of a biofilm and its architecture (Branda et al, 2005).
[4] In this, I discovered that I will not be a materials scientist, and I also reaffirmed that bacteria and evolution are mind-blowingly cool. All in all, a productive experience.
[5]In one of the best-titled articles of all time, “Biofilms: The Matrix Revisited”
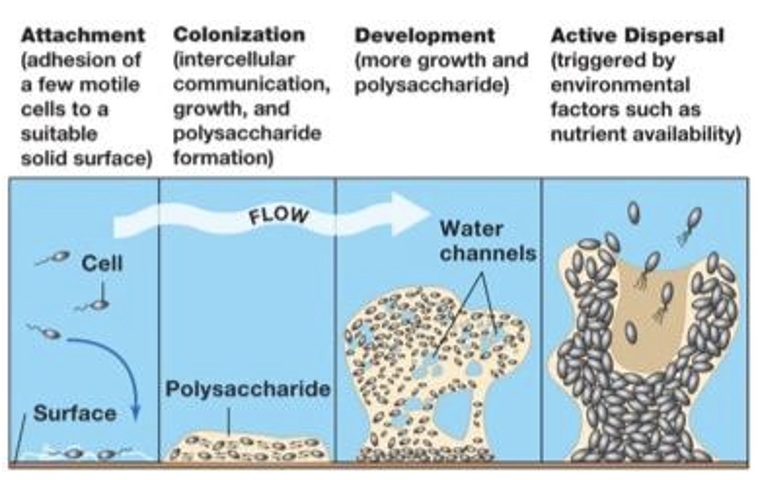
A diagram of biofilm formation, maturation, and dispersal (taken from the Microbiology, Immunology, and Molecular Genetics 301 class study guide at Michigan State University)
Biofilms have several ways of causing problems medically. Due to their enclosed structure and a social evolution between the component species, the communities are able to recycle nutrients and persist for long periods of time (Boyle et al, 2013). Diffusion of small molecules and antibiotics are slowed through the extracellular matrix encapsulating the biofilm, rendering the films largely resistant to antibiotics. Furthermore, the sequestering and cooperation between different bacterial species in a confined space leads to increased conjugation and antibiotic resistance. The “slime” of biofilms was thought to protect against immune cell penetrance, but recent studies have shown that the interaction between leukocytes (neutrophils, peripheral blood mononuclear cells, etc) and biofilms may actually promote and stabilize biofilm formation by stimulating the production of various cytokines (Walker et al, 2005; Chandra et al, 2007). Additionally, biofilms undergo repeated cycles of formation, maturation, and release, whereby the bacterial community can perpetuate itself by forming a new biofilm. Finally, biofilms contain within them “persister cells.” These cells, making up approximately 1% of the exponentially replicating cells during the formation of the biofilm but coming to play a much larger role in the later life of the biofilm, are in a state of dormancy and are almost impossible to kill. While not outright resistant to antibiotics, they are able to modulate their phenotypes to tolerate antimicrobial agents without undergoing genetic changes (Wood et al, 2016). The main model in the formation of these persister cells are toxin-antitoxin pairs which cause the cell to go into dormancy and protect itself by diminishing translation and the ability of cells to respond to stress. It is now thought that persister cells are the reason biofilms are so deadly to humans (Wood et al, 2016).
The formation of biofilms is an evolutionarily ancient and conserved process that is currently poorly understood. While there is a general understanding of how biofilms form and the evolutionary pressures that forced them to do so - sequestering of nutrients, efficacy of division of metabolic labor, increased protection from the exterior environment - this grey area between cell independence and multicellularity could hold the key to understanding how complex organisms such as ourselves evolved. How do these different species of cells contact one another? How do they maintain a balance between dependence and independence? The answer, other than evolution being incredibly complex and cool, is the concept of quorum sensing.
Quorum sensing is the regulation of gene expression in response to fluctuations in cell-population density. Certain bacteria with the capacity to perform quorum sensing release signaling molecules called “autoinducers,” such as acetylated homoserine lactones for gram-negative bacteria and processed oligo-peptides for gram-positive bacteria (Bryers, 2008). These molecules increase in concentration as a function of cell density. There is some threshold of minimal detection at which point the autoinducers cause genetic alterations. These genetic alterations induce a whole host of collaborative phenotypes, from symbiosis, conjugation, and competence to the production of virulence factors, antibiotic production, and motility. Just like everything else that is associated with biofilms, there is plenty of variation present in quorum sensing pathways. For example, some pathways have the ability to severely downregulate polymer production whereas other systems continuously secrete polymer. Evolutionary models have demonstrated that this, again, is due to the exquisite diversity in the composition of species contained within biofilms. If dispersal is necessary to access more nutrients (species are not able to recycle nutrients or are outcompeting crucial components of their ecosystem), the bacteria associated with these types of biofilms have evolved the ability to downregulate extracellular polymer production through quorum sensing. However, the energy expended in maintaining these pathways is not favorable in microorganisms present in chronic biofilm plaques, in which the strains involved can sustain stable nutrient equilibria (Nadell et al, 2008). Quorum sensing has been shown to be effective not only within a particular species but also across species and in some cases has been shown to elicit responses from host organisms (Miller and Bassler, 2001). This may hold a clue in the first steps of multicellular development and evolution. Not only that, but blocking autoinducers may be a way to prevent biofilm formation, disrupt this “social” behavior, and force microbes to exist in planktonic form, whereby they are susceptible/more reachable by antibiotics (Boyle et al, 2013).

“If you've done 6 impossible things this morning, why not round it off with breakfast at Milliways, the Restaurant at the End of the Universe?” (Adams, 1995) Today, I (1) successfully walked in sneakers without re-injuring my ankle, (2) did not freeze vegetables in my fridge, (3) learned more immunology than I thought was humanly possible in one day, (4) revived my dead computer, and (5) found the wallet that I thought was lost forever, along with (hopefully) (6) having taught you something new (seeing as you know everything already - or at least that’s my impression so far!). So please, Milliways, hold a seat for me.
REFERENCES
National Heart, Lung and Blood Institute. "What Causes Atelectasis?" National Institutes of Health. U.S. Department of Health and Human Services, 13 Jan. 2012.
Lawrence, Valerie A., Rahul Dhanda, Susan G. Hilsenbeck, and Carey P. Page. "Risk of Pulmonary Complications After Elective Abdominal Surgery." Respiratory Medicine 110.3 (1996): 744-50.
Asai, T. "Editorial II: Who Is at Increased Risk of Pulmonary Aspiration?" British Journal of Anaesthesia 93.4 (2004): 497-500.
Richter JE. Gastroesophageal reflux disease treatment: side effects and complications of fundoplication. Clin Gastroenterol Hepatol. 2013;11:465–471
Falagas, M. E. and Kasiakou, S. K. (2005), Mesh-related infections after hernia repair surgery. Clinical Microbiology and Infection, 11: 3–8.
Wenzel, R. P. "Health Care-Associated Infections: Major Issues in the Early Years of the 21st Century." Clinical Infectious Diseases 45.Supplement 1 (2007)
Bryers, James D. “Medical Biofilms.” Biotechnology and bioengineering 100.1 (2008): 1–18.
Choi, J.J, N.C. Palaniappa, K.B. Dallas, T.B. Rudich, M.J. Colon, C.M. Divino, Use of mesh during ventral hernia repair in clean-contaminated and contaminated cases: outcomes of 33,832 cases, Ann. Surg. 255 (2012) 176–180.
Ayala, Perla, Jeffrey Caves, Erbin Dai, Layla Siraj, Liying Liu, Ovijit Chaudhuri, Carolyn A. Haller, David J. Mooney, and Elliot L. Chaikof. "Engineered Composite Fascia for Stem Cell Therapy in Tissue Repair Applications." Acta Biomaterialia 26 (2015): 1-12.
Banthia, Ruchi, Rita Chandki, and Priyank Banthia. "Biofilms: A Microbial Home." Journal of Indian Society of Periodontology 15.2 (2011): 111
López, Daniel, Hera Vlamakis, and Roberto Kolter. “Biofilms.” Cold Spring Harbor Perspectives in Biology 2.7 (2010): a000398.
Costerton, J. W., G. G. Geesey, and K.-J. Cheng. "How Bacteria Stick." Scientific American 238.1 (1978): 86-95.
Branda, Steven S., Ã shild Vik, Lisa Friedman, and Roberto Kolter. "Biofilms: The Matrix Revisited." Trends in Microbiology 13.1 (2005): 20-26.
Lewis, K. "Multidrug Tolerance of Biofilms and Persister Cells." Current Topics in Microbiology and Immunology Bacterial Biofilms (2008): 107-31
Boyle, K. E., Heilmann, S., van Ditmarsch, D., & Xavier, J. B. (2013). Exploiting social evolution in biofilms. Current Opinion in Microbiology, 16(2), 207–212.
Chandra, J., T. S. Mccormick, Y. Imamura, P. K. Mukherjee, and M. A. Ghannoum. "Interaction of Candida Albicans with Adherent Human Peripheral Blood Mononuclear Cells Increases C. Albicans Biofilm Formation and Results in Differential Expression of Pro- and Anti-Inflammatory Cytokines." Infection and Immunity 75.5 (2007): 2612-620.
Walker, T. S., K. L. Tomlin, G. S. Worthen, K. R. Poch, J. G. Lieber, M. T. Saavedra, M. B. Fessler, K. C. Malcolm, M. L. Vasil, and J. A. Nick. "Enhanced Pseudomonas Aeruginosa Biofilm Development Mediated by Human Neutrophils." Infection and Immunity 73.6 (2005): 3693-701.
Bryers, J. D. (2008). Medical Biofilms. Biotechnology and Bioengineering, 100(1), 1–18.
Nadell, C. D., Xavier, J. B., Levin, S. A., & Foster, K. R. (2008). The Evolution of Quorum Sensing in Bacterial Biofilms. PLoS Biology, 6(1), e14.
Wood, Thomas K., Stephen J. Knabel, and Brian W. Kwan. “Bacterial Persister Cell Formation and Dormancy.” Applied and Environmental Microbiology 79.23 (2013): 7116–7121. PMC. Web. 20 Dec. 2016.
Miller, Melissa B., and Bonnie L. Bassler. "Quorum Sensing in Bacteria." Annual Review of Microbiology 55.1 (2001): 165-99.
Adams, Douglas. The Hitchhiker's Guide to the Galaxy. New York: Ballantine, 1995